by iphindia | Mar 16, 2016 | Blog, ATM, Latest Updates

Dr Praveenkumar Aivalli blog titled, ” What I learnt from my first health system research project ” published in BioMed Central
Starting my first research project
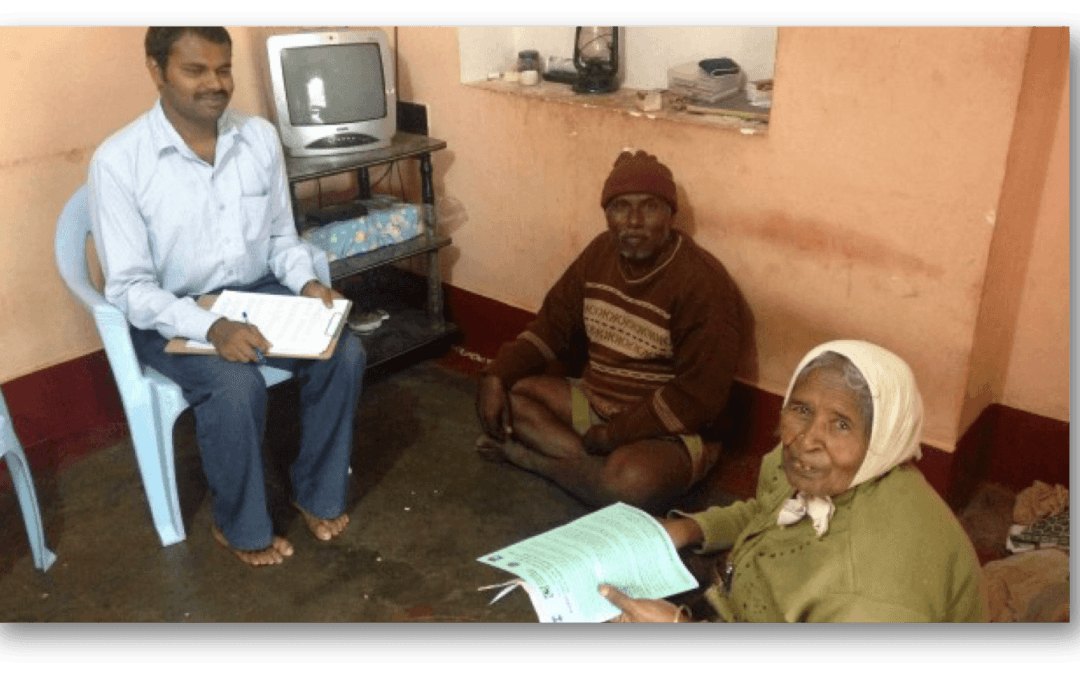
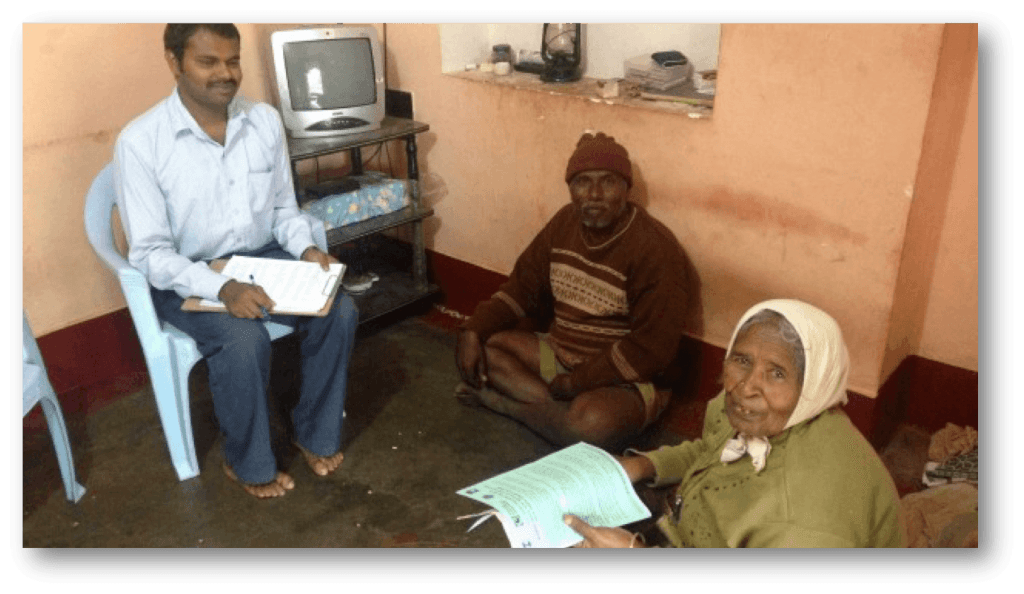
Back in 2013, I just stepped out of my university after getting my Master of Public Health degree, in no time I was given an excellent opportunity to work on a World Health Organization (WHO) funded health system research project in one of the reputed public health research institutes in Bangalore. It was the first research project of my public health career and as a new bee, I was buzzing with excitement and enthusiasm about the study.
The project was on improving NCD (Non Communicable Diseases) care at primary health centers in one of the districts in south India. It was a quasi experimental study trying to understand the impact of health system interventions through a baseline and end line household and facility surveys.
For better coordination, exposure and learning, I was placed in the study district. Having completed most of my education in the country, it was not that difficult for me to understand our country’s health system.
We visited more than 1000 families to get data on NCD care at the rural level, health seeking behaviors of NCD patients and their out pocket expenditures for NCD care.
The theoretical explanations from classrooms started fitting in its notches when I got exposed to the field during the early days of the project. I got the hang of the project fairly quickly and began preparing for the baseline survey in the year of 2013.
We visited more than 1000 families to get data on NCD care at the rural level, health seeking behaviors of NCD patients and their out pocket expenditures for NCD care. We also visited primary health centers and private pharmacies in the area to collect information on medicine availability.
To read more about Dr Praveenkumar Aivalli blog Click here
by iphindia | Oct 5, 2015 | Blog, ATM, Latest Updates

 Recently food security provisions in India has improved and not surprisingly the country is operating one of the largest food safety nets in the World. However regarding figures related to malnutrition particularly chronic malnutrition, the country is at very poor level. There are many challenges in implementation of food security schemes which hinders achieving desired outcomes of reducing malnutrition and the benefits reaching the actual poor.
Recently food security provisions in India has improved and not surprisingly the country is operating one of the largest food safety nets in the World. However regarding figures related to malnutrition particularly chronic malnutrition, the country is at very poor level. There are many challenges in implementation of food security schemes which hinders achieving desired outcomes of reducing malnutrition and the benefits reaching the actual poor.
Link to Manoj’s blog in Global Food Security….Click here
by iphindia | Sep 17, 2015 | Blog, ATM, Latest Updates

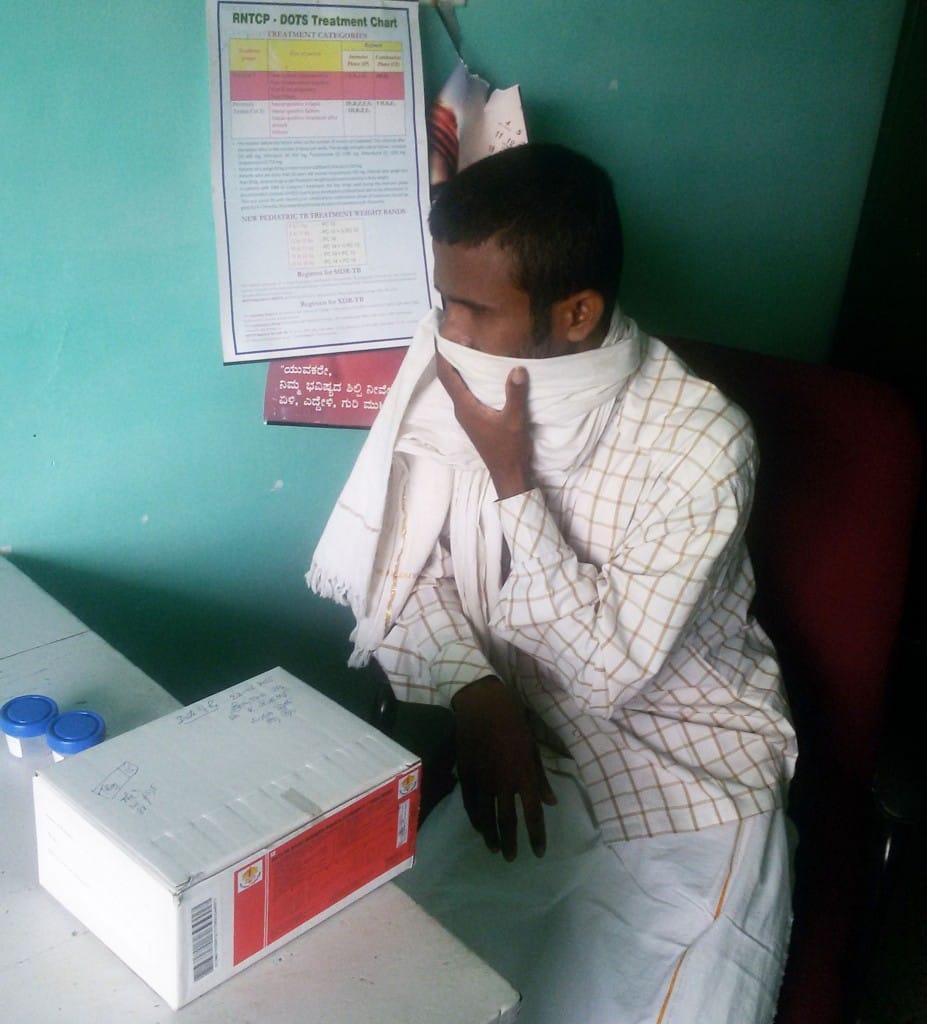
In India, tuberculosis (TB) is still a major public health problem. In this blog, the author reflects on the stigma and discrimination faced by TB patients and how it affects their health seeking behaviour.
Link to Munegowda CM blog in BMJ can be found here
by iphindia | Sep 16, 2015 | Blog, ATM, Latest Updates

Many of us are aware that the importance of breastfeeding in child growth and nutrition.But have we ever wondered, in a developing country like India where many mothers are now into formal or informal work, why is it important to have a mother-friendly workplace. World Health Organisation recommends exclusive breastfeeding for the first six months of baby’s life and early initiation of breastfeeding for protecting the child from various types of malnutrition.But unfortunately, breastfeeding has never been a central agenda in long history of health reform in India. Results are obvious. India houses larger number of malnourished children , twice as large as of Sub-Saharan Africa and five times larger than our neighbor China. Here is a blog which discusses what barriers exist and what can be done to bring back good breastfeeding practices into the list of larger sustainable goals for the country.
Link to Manoj Pati’s blog in BioMed Central can be found here
by iphindia | Aug 11, 2015 | Blog, ATM, Latest Updates

(Photo Credits- Biswarup Ganguly)
The World Health Organization (WHO) estimates that 1.24 million road traffic deaths occur every year globally. Of those, the majority (80%) of deaths occur only in middle income countries.Road traffic injuries are never considered a public health issue in India, rather reported as just any other event. India leads the world in terms of mortality from road traffic injuries.In India, road traffic injuries pose a significant public health challenge to the already overburdened health system, and hamper the economic development of the country.Three Es are important in preventing lots of death from road traffic injuries. Education in increasing awareness on road safety measures and behavior change among general public is important. Establishing and designing proper roads is more important. Most important is political will in stricter Enforcement of road safety laws.
Link to Manoj Pati’s blog in BMJ can be found from here.
by iphindia | Apr 27, 2015 | Blog, ATM
This article originally appeared on BMJ Blogs on April 24, 2015 under the same title.
Tobacco use is one of the single largest preventable causes of death and a leading risk factor for non-communicable diseases. The burden of tobacco related illnesses prompted the Government of India to initiate various measures for tobacco control. India adapted the WHO Framework Convention of Tobacco Control (FCTC) and passed the “Cigarettes and Other Tobacco Products (Prohibition of Advertisement and Regulation of Trade and Commerce Production, Supply and Distribution)” Act in 2003. The National Tobacco Control Program (NTCP) was launched in 2007-08 and it listed a wide array of regulatory activities for tobacco control, including setting up the National Regulatory Authority (NRA), state and district tobacco control programmes, public awareness campaigns, establishment of tobacco testing laboratories, prohibition of smoking in public places, prohibition of advertisement, sponsorship and promotion of tobacco products, prohibition of sale of tobacco products near educational institutions, and regulation of health warning in tobacco products packs.
Even after having active tobacco control programmes for well over a decade, we see that the focus is mainly on preventive measures such as educational campaigns and banning tobacco usage in public places. Though the National Tobacco Control Program recognized tobacco cessation as an important component and a critical step in controlling tobacco related mortality and morbidity, cessation activities have still not kept pace with other tobacco control activities. Less than half of the states under the programme have established tobacco cessation facilities at a district level. The recent ban of smokeless tobacco products was a major development in the history of tobacco control in India. A few state governments have taken other proactive steps towards tobacco control including declaring those states as smoke free. The latest policy debates are on banning the sale of loose cigarettes and increasing the legal age to buy cigarettes from 18 years to 25 years. While these efforts go a long way in tobacco control, which need to be appreciated, it also raises an important question: what services are available for a large number of regular users who require assistance to quit the tobacco use? It is interesting to note that while many of these states boast of being tobacco free, they are neglecting a vast number of active users who may need assistance to quit. It is estimated that around about 40% of tobacco users want to quit at any given point in time. A handful of exclusive Tobacco Cessation Centers (TCCs), attached to either medical colleges or tertiary care hospitals cannot guarantee access to millions of users who will require cessation services. Though there are some isolated private and Non-Governmental Organisation (NGO) initiatives, they are very limited in number and thus have very minimal outreach and impact.
In 2001, the National Human Rights Commission (NHRC) pointed out that India’s tobacco control initiatives are not effective enough and it violates the rights of tobacco users in many aspects including the right to access tobacco cessation programmes (as part of right of health). It was recommended that along with more effective information, education, and communication programmes on the effects of tobacco, assistance for tobacco cessation should be integrated into healthcare services to ensure access. Tobacco users are often faced with a counter argument saying “it is question of personal choice.” But in the case of a country like India, we see that tobacco users often do not have adequate information about the harmful effects of tobacco products. The latest global adult tobacco survey reported that only 50% of users were aware of the harmful effects of tobacco. It found that tobacco usage is higher among the disadvantaged and less educated, who may not be well informed and may not be able to make such conscious decisions.
What next?
It is evident that tobacco cessation has not received enough attention in our tobacco control programmes and often gets sidelined for various reasons, including resource crunch. So we need to think of alternative/additional strategies to reach out to more people and in a more sustainable, cost effective way. One possible solution is to integrate cessation activities into formal health services. While looking at the feasibility of integration at a primary care level, the major challenge is the shortage of human resources. However, it would be feasible to assess tobacco usage, and provide brief counseling and referral. Routine assessment of tobacco usage and brief counseling is known to have a positive effect on users. Comprehensive tobacco cessation services need to be made available in district and Taluka hospitals in order to cater for the vast number of users. Health workers, who are often the first point of contact for patients, can also play an important role in tobacco cessation counseling. Due to its prominence, the private healthcare sector can also play a crucial role in tobacco cessation.
Another area that needs attention is training health professionals in tobacco cessation. Often we see that medical practitioners and health workers are not aware of the harmful effects of tobacco and do not have the necessary skills to provide cessation services including counseling. One way to do this is to include tobacco related issues and its management in the medical curriculum and CME. The training has to be extended to different allied medical practitioners such as dentists and health workers as they come across more people using tobacco. Training on tobacco cessation strategies should also be imparted to teachers in school and colleges and “tobacco and its harmful effects” should be introduced as a topic in the school curriculum.
Telephone helplines have played a major role in tobacco cessation in the West. This can be tried out as a more cost effective intervention method. Innovative measures such as mobile apps and peer support platforms using social media could also be tried out as additional strategies.
Written by – Maya Annie Elias, Faculty member at the Institute of Public Health, Bengaluru.


 Recently food security provisions in India has improved and not surprisingly the country is operating one of the largest food safety nets in the World. However regarding figures related to malnutrition particularly chronic malnutrition, the country is at very poor level. There are many challenges in implementation of food security schemes which hinders achieving desired outcomes of reducing malnutrition and the benefits reaching the actual poor.
Recently food security provisions in India has improved and not surprisingly the country is operating one of the largest food safety nets in the World. However regarding figures related to malnutrition particularly chronic malnutrition, the country is at very poor level. There are many challenges in implementation of food security schemes which hinders achieving desired outcomes of reducing malnutrition and the benefits reaching the actual poor.