
by iphindia | Mar 16, 2016 | Blog, ATM, Latest Updates

Dr Praveenkumar Aivalli blog titled, ” What I learnt from my first health system research project ” published in BioMed Central
Starting my first research project
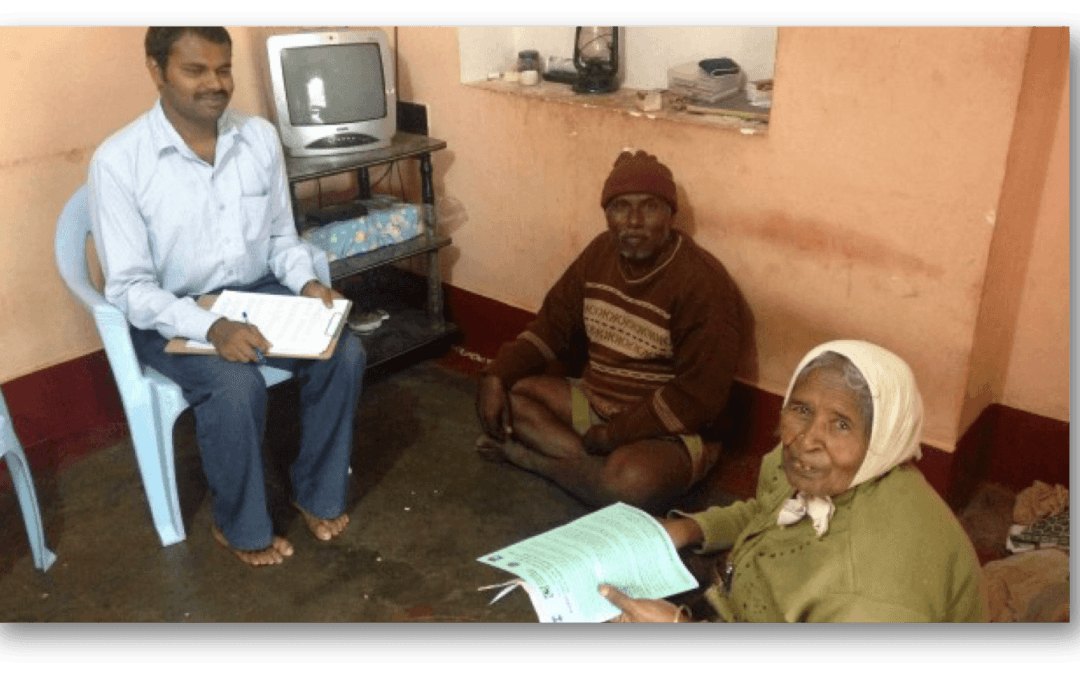
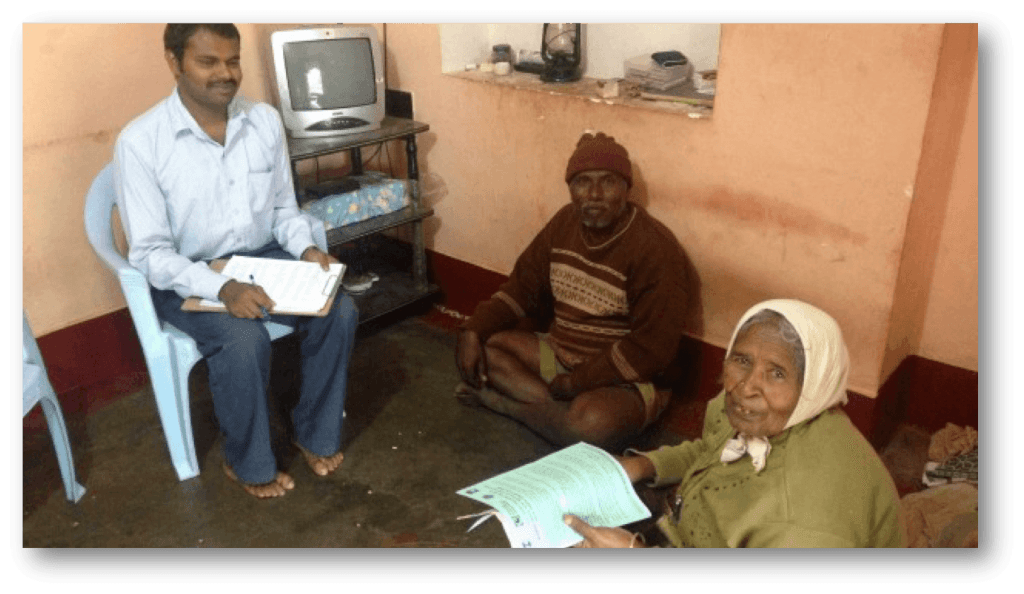
Back in 2013, I just stepped out of my university after getting my Master of Public Health degree, in no time I was given an excellent opportunity to work on a World Health Organization (WHO) funded health system research project in one of the reputed public health research institutes in Bangalore. It was the first research project of my public health career and as a new bee, I was buzzing with excitement and enthusiasm about the study.
The project was on improving NCD (Non Communicable Diseases) care at primary health centers in one of the districts in south India. It was a quasi experimental study trying to understand the impact of health system interventions through a baseline and end line household and facility surveys.
For better coordination, exposure and learning, I was placed in the study district. Having completed most of my education in the country, it was not that difficult for me to understand our country’s health system.
We visited more than 1000 families to get data on NCD care at the rural level, health seeking behaviors of NCD patients and their out pocket expenditures for NCD care.
The theoretical explanations from classrooms started fitting in its notches when I got exposed to the field during the early days of the project. I got the hang of the project fairly quickly and began preparing for the baseline survey in the year of 2013.
We visited more than 1000 families to get data on NCD care at the rural level, health seeking behaviors of NCD patients and their out pocket expenditures for NCD care. We also visited primary health centers and private pharmacies in the area to collect information on medicine availability.
To read more about Dr Praveenkumar Aivalli blog Click here
by iphindia | Mar 11, 2016 | Latest Updates
Erlyn Macarayan, an Emerging Voice of 2014 shares her reasons as to why you should apply for Emerging Voices for Global Health 2016! Apply now! Last date for application: March 20th 2016
Emerging Voices for Global Health (EV4GH) is an innovative multi-partner blended training program for young, promising and emerging health policy & systems researchers, decision makers and other health system professionals with an interest in becoming influential global health voices and/or local change makers. See http://www.ev4gh.net for details.
See http://www.ev4gh.net for details.
In 2016, continuing with the tradition of partnering with significant health systems research symposium, we have a new edition of EV4GH in close association and partnership with the 4th Global Symposium on health systems research, organised by Health Systems Global. See http://healthsystemsresearch.org/hsr2… for details.
See http://healthsystemsresearch.org/hsr2… for details.
The symposium will take place from 14-18 November, 2016 at Vancouver, Canada.
by iphindia | Mar 3, 2016 | Latest Updates
Sheila John from Sankara Nethralaya, Tamil Nadu,shares his experience at the e-learning workshop, “Get Started, Keep Moving” hosted by Institute of Public Health, Bengaluru & Institute of Tropical Medicine, Belgium. The workshop acquainted participants with various distance/blended formats.
I am a consultant ophthalmologist and Head of Telemedicine, Multimedia and E-‐Learning and working in Sankara Nethralaya a pioneer eye care Institution located in Chennai, TamilNadu, India. I have contributed to the content development in Multimedia and E-‐Learning departments
by iphindia | Mar 3, 2016 | Latest Updates, post_slider
Dr.Roopa Devadasan , took a session on team building for visiting MPH students from Rajiv Gandhi Institute of Public Health. The session was also attended by IPH staff members.
by iphindia | Mar 3, 2016 | Blog, Latest Updates
Rashtriya Swasthya Bima Yojna (RSBY) is a health insurance scheme, implemented by the Ministry of Labour and Employment, Government of India. The objective of this scheme is to provide protection to families below poverty line (BPL), against illnesses which involve hospitalisation. Currently, it covers beneficiaries’ families up to Rs 30,000 for most of the diseases that require hospitalization. In a BPL family, up to five members are eligible to get enrolled in the scheme and the government pays the premium of this policy to the insurance company. Each enrolled member of the scheme gets a biometric enabled smart card (SC), in which the basic personal details, photographs and thumb impression are stored. Beneficiaries need to present this smart card at the empanelled hospital to avail cashless treatment. As per the guidelines of the scheme, the smart card is issued at the time of enrolment itself, so that the beneficiary can start availing the benefit of the scheme immediately after the enrolment.
RSBY has been implemented in the state of Karnataka from 2009 and as per the official estimates, about 59% of BPL families have been enrolled in the scheme. I got an opportunity to witness an RSBY enrollment camp and in this blog, I would like to share my experience of interacting with the personnel involved in the camp. Once the camp started, the computer operator started taking photos and thumb impressions of the beneficiaries, but I noticed he was not providing the SC and Empaneled Hospital List (EHL) to them. Upon enquiring with the computer operator and his higher authority as to why the beneficiaries were not being given the SC and EHL, I instantly received a response that there was some technical issue. I pursued the matter further, to which the computer operator replied that the EHL was out of stock and that “if the cards were printed and provided at the time of enrolment they will not able to enrol more people thus not being able to reach the day’s target’’. He went on and clarified that due to this, they enroll the eligible people first, and will distribute the printed card along with list of hospital empanelled under the scheme after 10 days to beneficiaries through ASHA. His answer did not convince me completely, but I had no option other than to wait and see if the beneficiaries received their cards.
 After a month of enrollment, I checked with few ASHAs if the SCs have arrived, to which they replied that neither had they received any cards nor any documents. The whole incident surprised me! I continued to keep in touch with the ASHAs and enquire if they had received any of the cards. After three months, I found out that the cards were given to the ASHAs but they were less in number when compared to the enrolled beneficiaries. As per the list, the number of beneficiaries enrolled were 648 but only 500 cards were provided. Later, when I asked the ASHAs if they had distributed the cards, they said that they had not. They went on to tell me that as per the contract between ASHAs and Third Party Administrator , the ASHAs should get an incentive of Rs.7 per card; since they did not receive this incentive from the agency, they kept the cards with them instead of distributing them to the beneficiaries.
After a month of enrollment, I checked with few ASHAs if the SCs have arrived, to which they replied that neither had they received any cards nor any documents. The whole incident surprised me! I continued to keep in touch with the ASHAs and enquire if they had received any of the cards. After three months, I found out that the cards were given to the ASHAs but they were less in number when compared to the enrolled beneficiaries. As per the list, the number of beneficiaries enrolled were 648 but only 500 cards were provided. Later, when I asked the ASHAs if they had distributed the cards, they said that they had not. They went on to tell me that as per the contract between ASHAs and Third Party Administrator , the ASHAs should get an incentive of Rs.7 per card; since they did not receive this incentive from the agency, they kept the cards with them instead of distributing them to the beneficiaries.
This is not an isolated episode. Studies have shown issues with enrollment and card disbursement as major factors affecting the utilization of the scheme. Poor awareness of the scheme in the community is another major issue, which needs to be addressed. All these experiences show that monitoring activities of the scheme needs to be strengthened. The enrolment camps are great platforms for creating awareness about the scheme. Sound IEC activities along with good governance of the scheme will go a long way in improving access to healthcare for the poor.
Santosh M Sogal is Research Officer at Institute of Public Health, Bengaluru, shares his experiences and views on RSBY, the national insurance scheme of India.
Disclaimer: IPH blogs provide a platform for staffs to share their reflections on different public health topics. The views expressed here are solely those of the authors and not necessarily represent the views of IPH.
by iphindia | Feb 25, 2016 | e-Learning workshop 2015 Interview videos, Latest Updates
Piyush Gautam from Dr. Rajendra Prasad Government Medical College, Himachal Pradesh, shares his experience at the e-learning workshop, “Get Started, Keep Moving” hosted by Institute of Public Health, Bengaluru & Institute of Tropical Medicine, Belgium. The workshop acquainted participants with various distance/blended formats.
I am presently working as Assistant Professor, Pediatrics at Dr Rajender Prasad Medical College, Kangra at Tanda since 2011. I did my MBBS from Indira Gandhi Medical College, Shimla and my Post Graduation from PGI Chandigarh. I have served at various peripheral and district hospitals in our state prior to joining the Medical College. My areas of interest are Emergency Medicine and Intensive Care. I am looking after the Nutrition Rehabilitation Centr for severe acute malnutrition in our Department. I have been the co-‐guide for the thesis of two post graduate students. I am a member of the Medical Education Unit of our College, having done the Basic Course and presently pursuing the Advanced course in Medical Education. I am working with Dr Vivek in developing a Family Medicine Certificate course for MBBS doctors.





 After a month of enrollment, I checked with few ASHAs if the SCs have arrived, to which they replied that neither had they received any cards nor any documents. The whole incident surprised me! I continued to keep in touch with the ASHAs and enquire if they had received any of the cards. After three months, I found out that the cards were given to the ASHAs but they were less in number when compared to the enrolled beneficiaries. As per the list, the number of beneficiaries enrolled were 648 but only 500 cards were provided. Later, when I asked the ASHAs if they had distributed the cards, they said that they had not. They went on to tell me that as per the contract between ASHAs and Third Party Administrator , the ASHAs should get an incentive of Rs.7 per card; since they did not receive this incentive from the agency, they kept the cards with them instead of distributing them to the beneficiaries.
After a month of enrollment, I checked with few ASHAs if the SCs have arrived, to which they replied that neither had they received any cards nor any documents. The whole incident surprised me! I continued to keep in touch with the ASHAs and enquire if they had received any of the cards. After three months, I found out that the cards were given to the ASHAs but they were less in number when compared to the enrolled beneficiaries. As per the list, the number of beneficiaries enrolled were 648 but only 500 cards were provided. Later, when I asked the ASHAs if they had distributed the cards, they said that they had not. They went on to tell me that as per the contract between ASHAs and Third Party Administrator , the ASHAs should get an incentive of Rs.7 per card; since they did not receive this incentive from the agency, they kept the cards with them instead of distributing them to the beneficiaries. 

