by iphindia | Jan 26, 2015 | Blog, Education, Latest Updates
As part of Dr.Vijayashree’s PhD( Public Private Partnership in TB Care, Tumkur District), all the lab technicians working in the Designated Microscopic Centres of Tumkur district were trained (11.12.14) at District TB Centre, Tumkur city.
They were trained on the following:
1) DTO and MO-TB control explained about the project, research activities and the tools to increase the involvement of Private health sector providers in the National TB control Programme.
2) The critical role of lab technicians in involving the Private health sector providers in the National TB control Programme was explained. They were trained on how to document the source of referrals of patients who reach labs to get their sputum examination and how to use the study tools.
3) They were also trained on how to report the contribution of Private health sector providers in the National TB control Programme using Annexes

by iphindia | May 20, 2014 | Blog, Urban Health Action
Author: Dr Mrunalini
I am pretty well known in the country and constantly have a presence in news making headlines against the multibillion Pharmaceutical industries. I still struggle on a daily basis convincing people that I’m as good as the BIG BRANDS, and to start including me in their daily lives so to help them keep their diseases under control. This is a series of stories about me and a group of generics when we started our journey in K.G.Halli (Bangalore) through a primary care clinic in January 2014.
Every Monday, I sit there for few hours seeing people scan me with a close eye and have a skeptical look towards me and the idea of taking me home and start including me, to fight their war against the disease.
Along with me there are two doctors, two community health assistants bombarded with questions for being a generic drug, is there even a possibility of me being a generic drug?
The questions they encounter “Why is the color of the packet not green”? , Why do I have to take two medicines instead of one? , Why is it so cheap? Is it cheap because the strength is less? Do I actually help in controlling the disease? How can I be so affordable? Medicines for my disease always cost me a lot, how can the expenses suddenly be so less for a month, why are you people doing this work for the community? What do you get out of this? There are a lot of whys? There is lot of how can this be a real.

A lady sits across me , picks me up and says , this is not the same medicine for my disease, the shape is different, the cover is different, when I get two medicines in one tablet why should I take two separate tablets, will this cheap medicine help me control my disease?
The doctor sitting close by me answers with a comfortable ease and politely, that the packet color is different I agree, so is the shape. But the medicine which is required to cure your disease is inside this packet. Only the cover is different. The patient continues “but why can’t I get the combination?
Out in the community I’m an unspoken truth, or something which is never acknowledged, I’m a shadow amongst the big brands, the family physician when they see me pretend like I’m nobody. While the struggle continues, I choose to embark on a journey of my own in the community along with my dedicated team of doctors and community health assistants. I will introduce myself and promote myself that I too exist amongst the multibillion pharmaceutical industries, barring the fancy covering, huge promotion and marketing strategies.
Every journey begins with one small step, while I have embarked on this long journey, hoping it will be a successful in KG Halli.
by iphindia | Dec 13, 2013 | Blog
This is a story about a Primary Health Center (PHC) and a lady doctor. An ordinary centre in the way so many of our health centers in remote parts of the country are. This unremarkable PHC is located 52 km away from the district head quarters (HQ) and 36 km away from the taluk HQ. In Tumkur district of Karnataka. It is connected with poor roads and scarce public and private transportation. The PHC’s area of responsibility has 10,811 inhabitants distributed over 23 villages. The sex ratio is 976 female 1000 males and most people are engaged locally in agriculture while a few go to work in the district headquarter (HQ). The main agricultural products are paddy, ragi, coconut and arekanut. Local panchayat and sangaha members have good political influence at taluk and district level. And the villages are under strong political influences. The elected panchayat officials are no way supportive to the conduct or functioning of the PHC. But they are capable of putting pressure on government departments through their counterparts at the district level. This pressure tactics can lead to transfer or suspension of officials.

The PHC in our story has suffered due to lack of human resources since 2011, no doctor since 2 months, the ANM post lies vacant since the last 9 months, the pharmacist post since last six years, and alas…… two group ‘D’ posts are unfilled since four to five years.
The Medical Officer is by convention a doctor, so the post lay vacant in the PHC for two to three months. Meanwhile, a doctor working in a PHC in the neighboring district, who was born and brought up in Tumkur applied for this post in her home town. Apparently, she succeeded and got the transfer.
This new MO was disciplined, committed, and strict and self motivated. A good clinician, concerned about quality health care, she had experience in bringing about minor and major changes while staying in the HQ in her earlier PHC. Hence she joined this PHC and expecting to implement many changes.
As an initial step, she introduced a Token System for the Out patients department (OPD). Every day the centre sees 90 to 100 outpatients and it was difficult manage the crowd and provide quality service to each one. Her intention was that using tokens, patients should be able to consult a doctor with EASE COMFORT and PRIVACY. The system allowed the MO to give enough time for each patient, adequate for their needs. Eventually, when patients come out from the consultation room; they should have experienced the satisfaction of treatment.
Since many years, the PHC had not been reporting its information independently– it was reporting to the nearby PHC. The new MO wrote a letter to the Taluk Health Officer (THO) urging that the information be sent directly to him. He accepted, and with greater efficiency of team time, the information system was streamlined.
She made provision for all lab test materials to the PHC’s lab technician, thus precluding pregnant women going for ANC checkups to neighboring health facilities. She started visiting villages and anganwadis for regular health checkups and attending community level meetings. On one such visit, along with us, she observed that two to three open water tanks are providing the drinking water sources for villagers and may cause damage through infected water. She wanted to protect the water tanks, and sent a written complaint to the Gram Panchayat but no action was taken on it. She asked us if any NGOs were working on water and sanitation, wanting to co-operate in order to protect those water tanks so that villagers could drink safe water.
Along with these major changes, MO made some minor changes in the PHC, such as implementing the digital display of the information education communication (IEC) board. This board is where all patients can watch and learn about various national programmes. Earlier, the District Health Society (DHS) had distributed computers to all PHCs in the district but due to the erratic electricity supply to the PHC, the earlier MO had not brought the computer to the PHC. The computer lay unused in the THO office. Our new MO got the uninterruptedpower supply (UPS) device repaired and negotiated with THO about getting the computer back to the PHC. In conclusion, the computer reached its destination in working order. The MO also wanted to bring the PHC 24X7 working status; when deliveries could be conducted in the PHC avoiding much travel and hardship for pregnant women during labour.
While clearly she was trying to make some changes with existing resources, she was also facing many hurdles from some community members.
One day, a local Sangha related to ‘Kannada Rakshana Sangha’ (Karnataka Protection Sangha) thought to set up an idol on the occasion of Ganesh Festival, and they went to ask MO for contribution money. She refused to contribute money for the festival. One of the same sangha members, with political influence shouted at the MO, making allegations that she was taking money informally from the patients and using that money for car fuel. “And you denied to contribute the money for Ganesh festival “they shouted, but the MO ignored all this. But this man who shouted at the MO could not sit quiet; he went on to make a complaint against the MO to the DHO office. He reached the DHO office with one more person who was politically influential at the district level and lodged a complaint against the MO. They forced the DHO to issue a notice letter to MO. The DHO probably unaware of the ground reality combined with political pressure issued a notice latter based on the allegation made by the sangha member. The MO replied to the notice saying that she would not use the car from district head quarters…… and started using public transportation to reach the PHC.
Similar to this, one more incident happened in a different situation and on a different day in the PHC. As I mentioned earlier, the MO was so strict and disciplined that it was mandatory that all patients should take a token if they wanted to consult a doctor. Once, local political leader, knowing of this token system followed in the PHC, made direct entry to OPD consultation room. The MO did not recognize him and asked him to come in line with his token, but he shouted at her saying “I am a political leader belongs to XXX party and you should give the priority to us!” Unafraid, she denied his demand and asked him to come in line with the token. Embarrassed and wanted to take the revenge on the MO at a later time, when opportunities come; he kept all these things in the mind and went back.
One day, a patient with severe chest pain visited to the PHC around 10 am. Inopportunely, MO was on leave on that particular day and it was informed to THO over the phone. When patient reached the PHC, nobody was there, except group‘d’, non-medical staff. This staff called the 108 ambulance to transport the patient, but by the time the ambulance reached the PHC, unfortunately the patient died.
It appears that people who were angry with the MO for other reasons now got an opportunity to act. They went to a community member, succeeded in gathering several people and called for action against the MO. They succeeded in getting a higher authority to issue a suspension letter. The THO and DHO both visited the PHC to control and convince the crowd about the incident but they were unsuccessful in convincing the crowd. The crowd remained unmoved insisting that the District Commissioner (DC) come to the spot and the suspension order against the MO not be revoked… Eventually, the DC did come and tried to convince them about the circumstances around the death of the patient with chest pain. He did not succeed and finally issued a 3 month suspension letter to the MO with the consent of THO and DHO.
As a researcher who has spent two years in the taluk., I would like to state this…
A self motivated doctor tried to make some changes in a remote PHC in Karnataka using the minimal available sources and succeeded to some degree with no external and internal support in the system. Her attempt was to ensure that quality health care services were equally available to all, including the poor. She ended up travelling up and down 52 (one side) km in public transportation in order to prove a point. Eventually, the MO becomes a victim in a power-battle, and ultimately the community has lost good doctor in their PHC. The tail of the story is happier- the department revoked her suspension order and the MO has rejoined to department in another PHC, 10 km away from the district HQ, with good public and private transportation.
Bheemaray V M
by iphindia | Nov 15, 2013 | Advocacy, Blog
A shorter version of this article appeared on BMJ Blogs on October 31, 2013 under the same title. Co-written with Himabindu G L of IPH, Bangalore.
Much of the material remains unprocessed, or, if processed, unanalysed, or, if analysed, not read, or, if read, not used or acted upon
Robert Chambers
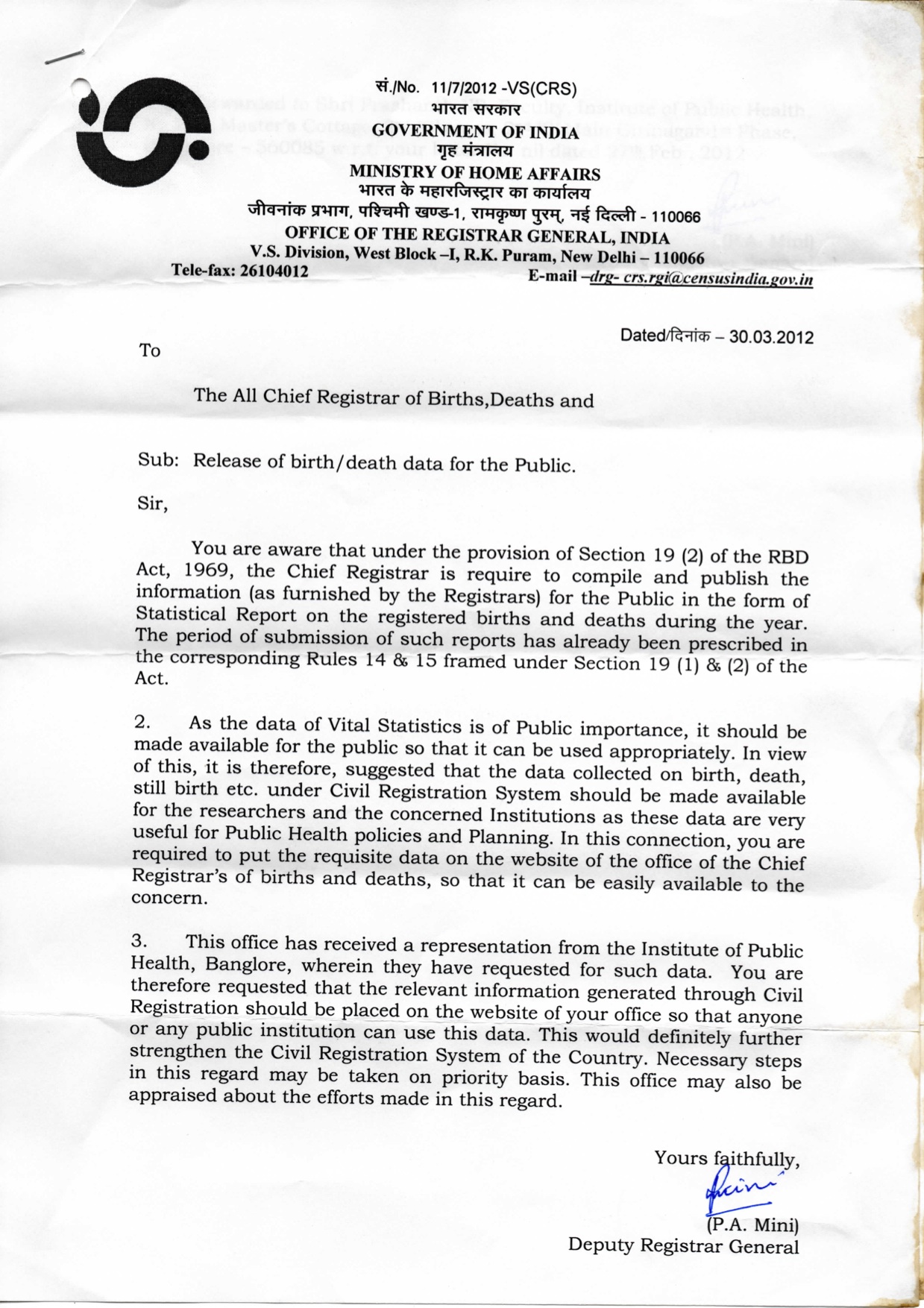
Basic demographic information forms the basis of policy, planning and public

The Registrar General of India promptly responded with this instruction to all states. But since then…
discourse. The system through which governments record vital events such as births and deaths is the civil registration system. Defined by the United Nations as “the continuous, permanent, compulsory and universal recording of the occurrence and characteristics of vital events”, it forms the basis for identity, citizenship and civil rights. Established perhaps first by Sweden, as early as 1631, its importance was globally recognised and more countries have worked towards establishment of efficient and comprehensive civil registration systems.
(more…)
![Juliet: We met, we supported and we lost…….& witnessed family getting dismantled?]()
by iphindia | Aug 11, 2013 | Blog, Latest Updates
This is not the first time we are writing about Juliet….but this will be the last blog we can write for her. A Call from the team member took me back to memory lane…
When we first time met young Juliet (name changed) she was pregnant with severe anaemia and reluctant to go for check-up (Why Juliet is reluctant to visit Public Hospital? https://iphindia.org/why-romeo-is-reluctant-to-visit-public-hospital/). Then we supported her through the pregnancy to delivery (May be it was dead before seeing the world https://iphindia.org/may-be-it-was-dead-before-seeing-the-world/). Not just during delivery in the hospital, also supported when she disappeared leaving nearly a month old baby at home. We got a call from one of the community member saying the baby will not make it if you don’t do something…we were not sure what is that “SOMETHING” we could do at that time!
When we went to see the baby….the baby was malnourished, with severe dehydration and  grandparents had decided to give the baby away! YES all they wanted was someone to look after that little boy. The sheer poverty and lack of social support can force people to take extreme steps….and added to that the substance abuse by all the elders in the family had not left space for responsibility and emotions. For the first time we witnessed whole community united to save little baby. After one month of intensive care at hospital, the baby was back in the safe hands of kind people in the orphanage.
grandparents had decided to give the baby away! YES all they wanted was someone to look after that little boy. The sheer poverty and lack of social support can force people to take extreme steps….and added to that the substance abuse by all the elders in the family had not left space for responsibility and emotions. For the first time we witnessed whole community united to save little baby. After one month of intensive care at hospital, the baby was back in the safe hands of kind people in the orphanage.
Few months later Juliet was pregnant for the second time and she wanted to have another child! I was shocked and angry….our advice not to conceive had not helped. But this time she was taking care of herself and was going for regular check-up. “She is matured madam” said field team member. I was wondering with no family support, what will happen to her and the baby this time! What should be our role…many more questions while her baby was growing in the womb! But we didn’t have to do anything this time….Juliet was in critical care unit.
 During a spat, a punch from her husband had caused head injury and she was unconscious in critical care unit and husband in Jail. After few days of struggle, doctors gave up…caller from the other side said “sorry madam Juliet died”!
During a spat, a punch from her husband had caused head injury and she was unconscious in critical care unit and husband in Jail. After few days of struggle, doctors gave up…caller from the other side said “sorry madam Juliet died”!
Few months ago Juliet’s mother-in-law also died and the community is requesting to leave her children in orphanage with Juliet’s baby! In less than two years we witnessed the whole family getting dismantled…Juliet’s baby in orphanage is doing very well, the only consolation we have. This is a story of one Juliet but I’m sure there are many more Juliet’s in our community who need support, guidance and a proper system to address social issues, which is lacking.
Dr Thriveni B S
https://iphindia.org/urban-health-project/